It is exciting to think that there may be new methods for those who struggle with pumping. I’m cautiously optimistic.
Suzanne Sanders here, IBCLC for another article review.
This pilot study “Flange Size Matters: A Comparative Pilot Study of the Flange FITS Guide Versus Traditional Sizing Methods.” was published in November 2024 in a peer reviewed journal. (1)
Before we jump to the results, let’s talk about the method. 36 participants were measured and fitted with two different flange sizes. One flange was chosen based on the Flange FITS method (which is a new, smaller-sized fitting) and one flange was chosen based on the fit instructions from their specific pump manufacturer (standard fitting). For one week, they pumped at least 3 times (averaged 4.62 times) using the standard flange size, and for one week they pumped at least 3 times (averaged 4.71 times) using the smaller flange size. Half the participants were randomly assigned to pump the first week with the standard fit and the following week with the smaller fit, while the other half of the participants did the opposite. They pumped with their own double-electric, non-wearable breast pump. They were instructed to pump roughly the same time of day, at least 2 hours after their last pumping or nursing session.
The study found that those using the standard flange had less milk output and less comfort than when they used the smaller flange.
What I found fascinating were these two graphs: Figure 4 and Figure 5.
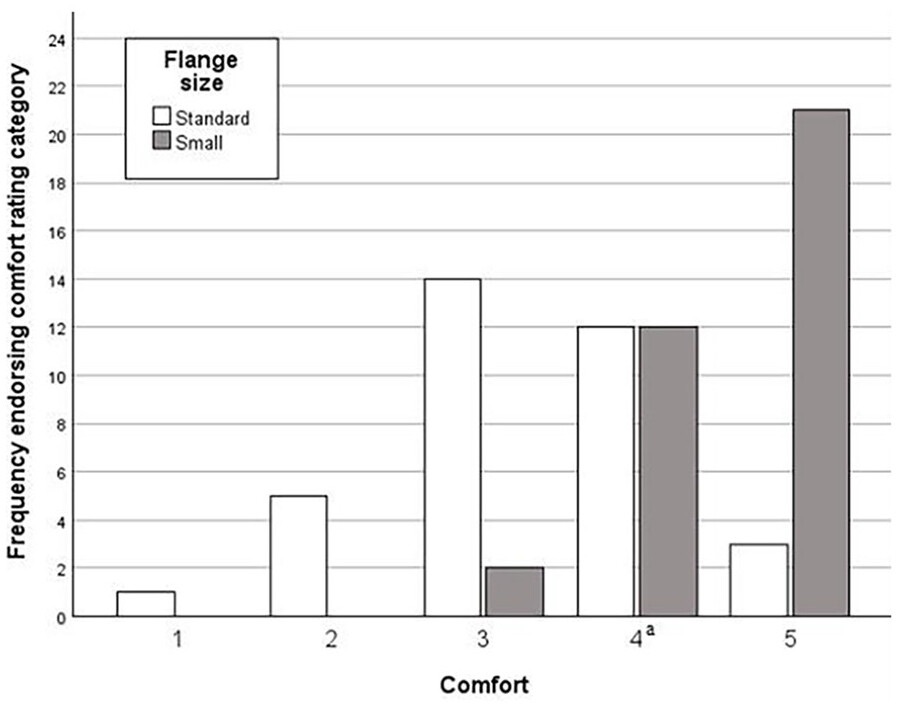
Figure 4 shows the patients’ reported comfort level. At the end of the week the participant pumped with the standard fit flange, they submitted one comfort rating, and at the end of the week they pumped with the smaller fit flange they submitted another comfort rating. The rating of 5 is ‘very comfortable or feels like nothing’ while the rating of 3 is ‘tolerable’. The average comfort rating for the standard size was 3.3, while the average comfort rating for the smaller fit was 4.5. For your in-the-workforce parent, or exclusively pumping parent, who has to pump multiple times a day, I imagine moving them up 1.2 points on the comfort scale could make a big difference in their breastfeeding journey.
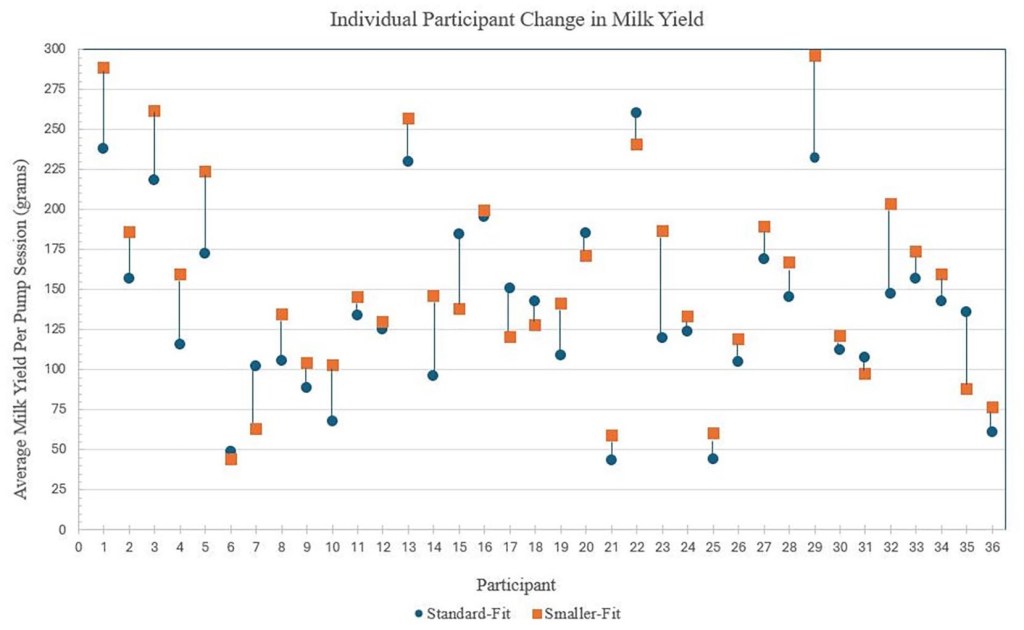
Figure 5 is also worth a look; this is the change in milk yield between the smaller fit (portrayed by the orange square) and standard fit (portrayed by the blue circle). What I really appreciate about this visual is the nuance amongst individual participants. The mean milk yield for the smaller fit was 153.2 grams, and the mean milk yield for the standard fit was 138.2 grams. You can see in this image that some participants noticed a decent increase when using the smaller fit, while some barely noticed a difference and some noticed a decrease in milk yield.
This study highlights the importance of a flange fitting being “an individualized process led by participant reports of comfort and milk yield.” I think Figures 4 and 5 support this idea. In the supplementary material for this article, you will find a brief guide about how to find the flange sizing for the Flange FITS model. What I find most fascinating about this method is how personalized it is to the individual. It takes trial and error in an appointment and collaboration between lactation professional and the pumping parent. They try multiple different flanges to find which size both produces the best milk sprays and feels the best. My biggest takeaway from this research article is just how personalized and nuanced it is to find the best flange for the individual.
What is important to remember is this is a pilot study, the first of its kind with a relatively small pool of participants. To my understanding, these results need to be replicated by ideally a larger and longer study before we can actually change our current practice and call it ‘evidence-based’. (See my below section What I Learned). Also worth mentioning – there is a very specific method for how the ‘smaller fit flange’ was chosen; it’s called the “Flange FITS” and the guide is free. Hint: it involves actually trying a few flanges out with the patient while they are pumping and collaborating with the patient, so if you’re curious about how to choose the smaller size for your patient: find the guide.
I’d love to hear your thoughts on the article after you read it – post in the comments below and let us know your credentials. I want your input whether you’ve been in the research field for 30 years or if this is your first time reading a research article.

What I Learned : Pilot Studies
I did some digging to learn what a pilot study actually means and what a pilot study can reveal. From my readings, a pilot study is not intended to address a hypothesis. So, pilot studies, in general, are not designed to ask the question ‘Does this intervention work?’ It instead addresses the question ‘Can we perform this experiment?’ When reading and interpreting a pilot study, that’s a HUGE difference. The pilot study can be very helpful when creating a full-scale study by helping to catch and reduce errors and problems that may be encountered in the full-scale study. (3)
One article I read states:
“Pilot studies should not be used to test hypotheses about the effects of an intervention. The “Does this work?” question is best left to the full-scale efficacy trial, and the power calculations for that trial are best based on clinically meaningful differences. Instead, pilot studies should assess the feasibility/acceptability of the approach to be used in the larger study, and answer the “Can I do this?” question.” (2)
The intention is for the nipple tip to ‘glide against the sides of the [flange] tunnel’. Is this going to increase the risk of nipple damage? In this study, there were no reported injuries, but they followed up with the participants after only 1 week of pumping (per flange). What length of follow-up time is needed to determine the safety of this new method?
One other question: In the supplementary material, The Flange FITS Guide states “A thin layer of coconut oil or nipple balm on the bend of the flange can increase comfort.” Do we have any evidence that applying oil or balm to the flange affects -or does not affect- the expressed milk that ends up in the bottle?
References
1. Anders LA, Mesite Frem J, McCoy TP. Flange Size Matters: A Comparative Pilot Study of the Flange FITSTM Guide Versus Traditional Sizing Methods. Journal of Human Lactation. 2024;41(1):54-64. doi:10.1177/08903344241296036
2. “Pilot Studies: Common Uses and Misuses” NIH National Center for Complementary and Integrative Health. Accessed 5/1/2025. Last Updated 5/1/2025. https://www.nccih.nih.gov/grants/pilot-studies-common-uses-and-misuses
3. Kistin C, Silverstein M. Pilot Studies: A Critical but Potentially Misused Component of Interventional Research. JAMA. 2015 Oct 20;314(15):1561-2. doi: 10.1001/jama.2015.10962. PMID: 26501530; PMCID: PMC4917389.